
On 24 November 2022 Ontario’s nursing unions warned that the public healthcare system was collapsing:
After several years of neglect, underfunding, and failure to improve staffing levels, the health system is now buckling under the weight of severe staff shortages, overcrowding, lack of surge capacity and the spread of COVID-19, a big and early surge in the flu and other respiratory illnesses.
From Ontario Nurses’ Association.
The Ontario Nurses’ Association is a federation of five nurses’ unions. In their press release the leaders of these unions explained that they had tried to get Premier Doug Ford to act, “But after weeks with no response, the unions say that Doug Ford is openly ignoring frontline workers and patients, and actively pushing the public health care system to collapse, by doing as little as possible to sustain it.”
Private Medical Companies
The nurses accused the Premier of more than neglect, stating that the government is breaking the system deliberately:
The five leaders expressed grave concern that Ford is using the crisis to drive his costly privatization agenda and warned that two-tier health delivery will make staffing shortages, wait times and patient outcomes even worse by competing for scarce staff and pulling them out of the public system, where wages have been cut.
How has the Ford government accomplished this?
Balancing the Budget on the Nurses’ Backs
This crisis did not begin yesterday. Years of successive budget cuts by Ford’s Tories and previous Liberal governments have reduced Ontario’s healthcare capacity by 7,300 Registered Nurses in the past ten years:
75 per cent of those RN positions — more than 5,500 — were cut from 2013 to 2016, a time when the former provincial Liberal government, led by Kathleen Wynne, tried to rein in health spending in an effort to balance the budget.
From Toronto Star, 18 May 2022
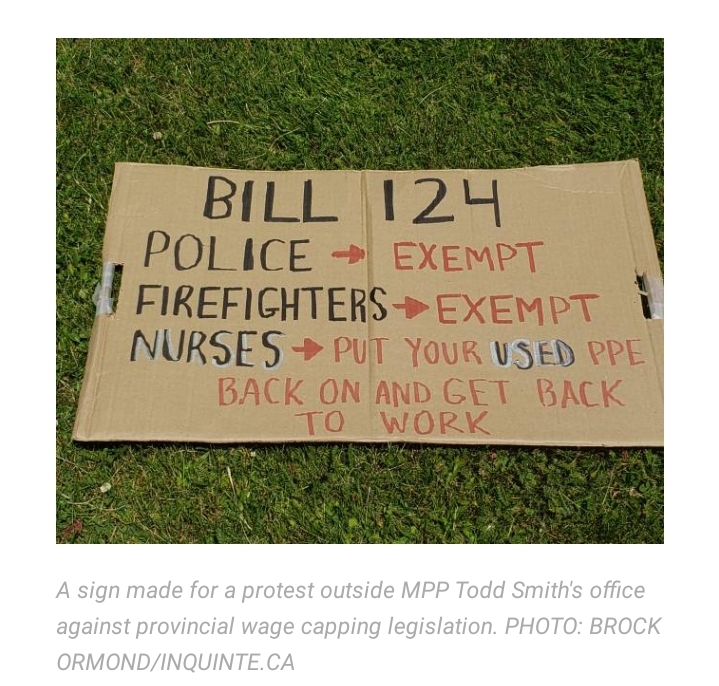
But Doug Ford’s Progressive Conservative Party (PCP) has pushed the system to its limit. A year after taking power the PCP passed Bill 124, the “Protecting a Sustainable Public Sector for Future Generations Act, 2019” into law. This law cut benefits, capped healthcare workers’ wage raises at 1% per year, and reduced full-time staffing. With inflation averaging 6% a year this means that Ontario nurses have suffered a 5% pay cut every year since 2018.
The government also refuses to hire more fulltime workers and has underfunded hospitals to the point that entire departments must shut down to keep the rest of the hospital running.
Bill 124, the wage suppression law, had a catastrophic effect on healthcare workers. In December 2020, the first “dark winter” of COVID-19, 34% of Registered Practical Nurses (RPNs) were considering leaving nursing. This grew to 47% of RPNs by 2022:
Eighty-eight per cent of RPNs said they have been impacted by the staffing shortages, with many facing “added stresses and increased isolation.”
From CTV News, 3 August 2022.
Specifically, seven in 10 said they have had to work more hours to cover staffing shortages, including 39 per cent who worked unpaid overtime hours at the end of their shifts.
In addition, six in 10 nurses said their mental health has deteriorated because of the stress regarding staffing shortages.
“I feel like we have to constantly rush residents and cut corners to get everything ‘done’ and decide between taking breaks and completing tasks for every shift,” an anonymous nurse wrote.
It’s not only nurses who are hit by the Tories’ plans to defund and privatize healthcare. Family physicians have been leaving Ontario in droves.
Shorting Ontario’s Family Doctors
From March to September 2020 3% of Ontario’s family doctors left their practices and “as of March 2020, nearly 1.8 million Ontarians did not have a family doctor and another 1.7 million Ontarians have a family doctor older than 65 years old.” In other words, 12% of Ontarians had no family doctor and 11.3% had one beyond retirement age.
As with the nurses, the Tories are accelerating the attrition of family doctors. During the COVID lockdowns doctors used telemedicine services to address clinic closures and staff shortages. The public health insurer, OHIP, had paid doctors for these calls as if they were regular visits. This changed on 2 December:
While fees for one-off visits were previously set at $37 for minor assessments and up to $60 for longer sessions, the changes cut those to $15 for phone calls and $20 for video sessions.
From Global News, “Virtual care platform sees exodus of doctors as result of Ontario fee changes”
A survey published on 17 November shows the destructive impact of Conservative policy on primary care doctors. With rising administrative costs and shrinking compensation, 20% of Toronto family doctors plan to close their practices in the next five years.
The pressures on primary care have become unbearable for the patients, their caregivers, and the actual structure of the system they work in. With the intensifying shortage of nurses and doctors comes an increasing number of patients who cannot secure an in-person appointment with their doctors. This has resulted in patients going to overcrowded ERs for basic care.
Faced with unmanageably large workloads family doctors are forced to de-enroll patients, some that they’ve had for decades, and there is no relief in sight:
Ontario’s Ministry of Health tells CityNews in a statement that the province has added more than 1,060 family doctors, though the ministry did not specify whether those are net-new positions, or simply replacements as doctors leave the profession.
From CityNews, “Ontario family doctors letting patients go as caseloads become unmanageable.” 7 December 2022
The Government addressed the looming primary care crisis on 21 November:
[A] recent memo, sent by the Ministry of health on Nov. 21, acknowledged that the province is dealing with a “difficult and complex” respiratory illness season and called on primary care doctors to “offer clinical services seven days a week, including evening availability, until further notice.”
From Global News, “Ford government asks primary care doctors to work at ‘full capacity,’ extend hours”
The Health Minister’s memo was a supposed attempt to shore up Ontario’s hospitals as they are battered by multiple epidemics. Her request to doctors (not an order; that would require the Government to act) is impossible to fulfill as many primary care clinics are already working extra hours, with unpaid overtime, while their own staff and resources are dwindling:
“We’ve had just as many people have to take time off for burnout. We’ve had people away that are sick. We’ve also lost nurses that work with us in our offices, just as we’ve seen in the hospital and acute care system,” Dr. Grill [Chief of Family Medicine at Markham Stouffville hospital] told Global News.
It is obvious that Health Minister Sylvia Jones is not making serious efforts to correct the crisis. Instead, she is encouraging exhaustion and systemic collapse to spread like a contagion.
What do the conservatives expect to happen to the nurses they’ve driven out of the profession? Where are underpaid and demoralized public healthcare workers supposed to go?
Private Sector Poachers
In Ontario it is illegal for certain public sector employers to compete with private sector contractors. The Conservatives’ Bill 124 bars the government from offering anything close to a competitive wage, leaving private contractors in control of the job market.
“If I were making $112 an hour and you were making $45, how do you think that would go over?”
Cathryn Hoy, president of the ONA. From Ottawa Citizen.
For years hospitals have used privately-owned staffing agencies to fill vacancies on short notice. These agencies were a minor part of the healthcare workforce until the COVID pandemic pushed hospitals and workers to their limits.
The agencies offer their temp staff as a premium service to the public healthcare system. The agency charges enough that they can take a profit while giving nurses two, possibly three times their regular wage. The appeal of an agency job is obvious, especially when wages are stagnating and cost of living is rising:
“Nurses making pretty much double what all the other nurses on the floor are making and the business that they work for is billing the hospital about four times what a nurse would be. So they’re actually paying four times the hourly rate for a nurse that the hospital is paying, which is abuse of health care funds,” Hoy said.
From CHCH, 18 August 2022
…
Hoy says she’s heard that one hospital’s nursing staff is 85% privately employed, something she says is an unsustainable model since the agency nurses are making anywhere between $80 to $112 an hour.
The agencies can afford to pay double the public wage because they bill it all to the hospital. The agency pays nothing out of its own pocket and charges the hospital for the cost of labor plus the agency’s fee. Private businesses like these also operate on the laws of supply and demand: as demand for temp staff increases, so does their price. The hospitals can’t really say no and, despite their limited budgets, must pay market rates for temp staff.
So, rather than retain staff and pay public nurses $80/hour, the Tories prefer that hospitals pay hundreds of dollars per hour to rent their own former staff.
As nurses quit the public staff to join the private labor market, the agency’s leverage over the hospital grows: the hospital is down by one nurse and the agency is up by one. As ONA president Hoy said, there are already cases where the private agencies have monopolies on healthcare labour.
By suppressing healthcare wages Bill 124 made it much cheaper for agencies to recruit from the public system. Their efforts to privatize the workforce are well underway and once the public system is gone they will have no reason to keep offering premium wages. The private monopolies will be free to dictate terms in the labour market: to slash wages, reduce work hours, and eliminate benefits. In other words, the private bosses will use all their usual tricks to suppress the workers.
The Children’s Pandemic
This year all of the major news outlets have warned of a “tripledemic” expected before the winter. Three viral epidemics were expected to overlap and compound each other’s destructive effects: COVID-19, Respiratory Syncitial Virus (RSV), and Influenza. RSV is a virus which is usually mild, causing symptoms similar to a common cold. Since 2021 it has had an increasingly severe effect and has hospitalized hundreds of children.

The news media’s consensus on the cause of the tripledemic is that there is an “immunity gap” created by the COVID restrictions of the past two years. This common sense argument says that children were robbed of the opportunity to gain immunity to RSV and the flu because they were not exposed to viruses for a year and a half; their immune systems have no memory of RSV and cannot fight it.
Common sense arguments like these gave us the utterly failed herd immunity “strategy” for COVID, based on the assumption that getting infected with SARS-COV-2 would provide immunity against future infections. The ongoing and intensifying pandemic is proof that these arguments are false.
The evidence says that COVID damages the immune system for a year or even more after infection. T cells are expended on clearing the virus out of the system and the regeneration of “naive” T cells is inhibited. Naive T cells are those which have no “memory” of a virus or bacterium. They are blank slates ready to identify and fight a new infection. When they are suppressed the body struggles to develop immunity and stays sicker, longer with each new infection.
Even mild COVID destroys critical cells of the immune system and inhibits production of Interferon-alpha, a protein which is essential to catching and destroying viruses.
Recent data from Denmark shows that children’s immune systems are actually stronger if they do not get RSV: children who avoided it because of COVID lockdowns in 2020 an “immunity credit“.
The final element of the tripledemic had arrived by 5 December as hospitals reported an unusually early and intense flu season. The flu will not be the end of this cycle. Evidence shows that “Long Influenza” afflicts 30% of flu patients, Norovirus and Strep A are spreading in flu-ravaged England, and a University of Glasgow study has identified a hybrid of RSV-Influenza:
[R]ather than competing with one another as some other viruses are known to do, they fused together to form a palm tree-shaped hybrid virus – with RSV forming the trunk, and influenza the leaves.
…
“We are talking about viruses from two completely different families combining together with the genomes and the external proteins of both viruses. It is a new type of virus pathogen.”
From The Guardian, “Immune system-evading hybrid virus observed for first time.” 24 Oct 2022
COVID leads to worse RSV which leads to worse Influenza, and all three lead to weakened immune systems and secondary infections. One infection compounding on another and another…
Essential drug shortages

In November all 4 domestic producers of the antibiotic amoxicillin reported that they’d run out of supplies. This news came in the middle of an ongoing national shortage of children’s fever medicine. Both shortages resulted from the tripledemic as people rushed to treat symptoms of respiratory viruses and secondary, bacterial infections in children.
On November 15th a pharmaceutical industry rep explained the shortage of children’s Tylenol to Parliament:
He said drugmakers had already planned for higher-than-normal demand for this year’s cold and flu season, but that demand started to rise back in the spring ahead of expectations.
From Toronto Star.
Fevers cannot be controlled and common infections progress to dangerous stages. Children are being hospitalized at rising rates because their illnesses can’t be treated at home or by a family practitioner.
The drug shortage coincides with two other major developments: the early surge of RSV in the spring and the first ER shutdowns in March.
Hospital shutdowns
In 2022 Ontario began to suffer rolling emergency room closures. These started in March, the first time it had happened since 2006.
The once rare event became commonplace in 2022 as more and more hospitals reported that dangerously low staffing had made it impossible to treat patients.
Toronto Star reported that from 2 July to 16 September Ontario hospitals endured 86 closures totalling 1700 hours of lost ER time.
ER closures have been clustered around long weekends and holidays: ONA reported 20 closures during the August long weekend “due to catastrophic staffing shortages.”
In the national capital Ottawa, four ERs and medical facilities were closed during the September long weekend. The reason: “staffing shortage.”

On 7 October a rural hospital in Bruce County closed its ER until December, saying it is unable to maintain staffing or afford private nursing agencies:
[T]he hospital has been relying on agency nurses to fill shifts, but that solution is costly and not ideal. It said agency nurses are “not committed to our hospital sites,” and are paid more than staff nurses, making them feel undervalued.
From Global News.
With so many erratic hospital closures it is impossible for an already-thin ambulance fleet to transport patients to the nearest Emergency Room. “Level Zero” events have become increasingly common; Level Zero means that there are no ambulance crews available to take new emergency callers into the hospital. Ottawa saw 750 events in 2021 and 1000 Level Zeros before the end of October 2022.
When the nearest open ER is five hours away, the medical helicopters are needed. But they are also underpaid and unable to maintain adequate staffing, all while the tripledemic sends record numbers of children to the air ambulance.
Pulling the Plug
The tripledemic has torn through the anemic healthcare system, bled dry by the Doug Ford Tories:
Sick children are being flown by helicopter to American ERs.
Adults and children with emergency heart surgeries are being delayed for weeks.
ER wait times are as high as 45 hours, averaging 12 hours.
The Conservatives were hollowing out the healthcare system despite warnings of an imminent outbreak from top medical officers. This predictable surprise arrived as the tripledemic.
The Ford government’s failure to act is not incompetence or negligence.
Keeping students in school
The Ford Government has a singular fixation of keeping schools open and kids in physical classrooms. The obvious reasons are not that they care about the quality of education or about children missing out on lessons; if the Tories cared about that then they wouldn’t be defunding the school system. Instead, the obvious reason is that this Government sees schools as “glorified daycares” that keep kids in one place so their parents can work and make profits for their bosses.
2020’s COVID-induced school closures were intolerable to the Tories. Public schools had been shut down 12 March 2020 and did not fully reopen until 15 May 2021. Millions of working parents has lost hundreds of millions of hours of productivity and their bosses were mad.
Ontario’s lockdown ended ten days after Health Canada approved COVID vaccines for youth 12 and up, and only a week before the country reached the milestone of giving 50% of adults their first dose. With “shots in arms” the Government insisted that it was safe to put students in school.
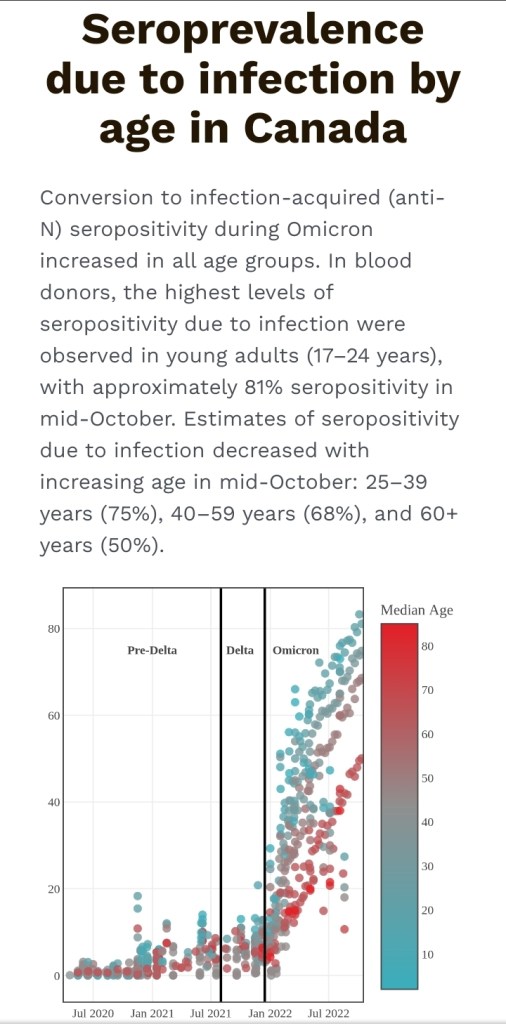
The school lockdown had protected children from their most likely vector of COVID infection. A study of data from the period just before the end of the lockdown showed that youth COVID seroprevalence (proportion of the population with antibodies for a virus) was very low, only 3.4%:
The overall seroprevalence of SARS-CoV-2 antibodies was 3.4% among children and youth 1 to 19 years of age between November and April 2021,” explains Mr. Gravel. “As vaccines had not yet been distributed to this age group at the time of the survey, nearly all of these children and youth had antibodies due to a previous infection. In comparison, 2.9% of Canadians 20 to 59 years of age, and 1.4% of Canadians 60 years of age and older, were found to have antibodies due to a past infection.”
From COVID-19 Immunity Task Force.
On January 3rd 2022 the Government announced that they would be reverting to Step 2 of the “Roadmap to Reopen,” requiring public facilities to close and commercial facilities to close or operate at reduced capacity. Schools would remain closed and students would attend online learning. This was to slow the spread of the extremely contagious Omicron variant, which the announcement acknowledged could overwhelm the healthcare system faster than any previous COVID wave.
Despite their own warnings the Government reopened schools to in-class learning on 17 January. With two weeks between the Step 2 announcement and the reopening of schools there was plenty
The Government had reached this decision at the end of December 2021 and refused to change it even when they recognized the threat of the Omicron strain. The Tories insisted that schools must reopen and stay open regardless of the danger to students’ health and safety. Their further decision to exempt schools from masking requirements guaranteed that an enormous outbreak would hit Ontario’s children and youth.
By October 2022 the COVID seroprevalence among Ontario’s youth had risen from 3.9% to 81%.
The final mask mandates were lifted on 11 June, expanding the tripledemic to hospitals, homeless shelters, elder care homes, and public transit.
Letting RSV run rampant
The Government had ample warning of the RSV epidemic. The virus had previously been a nuisance but in 2021 it began causing outbreaks of severe illness.
The CDC had issued an RSV warning on 10 June 2021 based on a March surge in the southern USA. This warning was cited by a paper published in the Canadian Medical Association Journal on 26 July, “Potential resurgence of respiratory syncytial virus in Canada.” Before the end of 2021 the news media were reporting outbreaks of RSV across the northern hemisphere.
The Ministry of Health certainly had access to all of this information and more. Nevertheless the Government did not prepare for the epidemic. No effort was made to retain crucial staff, to relieve the pressures on the system, to reduce the transmission of viruses, or to stockpile essential medicines.
The CDC reported that rates of RSV-associated hospitalizations began to increase during late spring 2022 and continued to increase through the summer and into early fall.
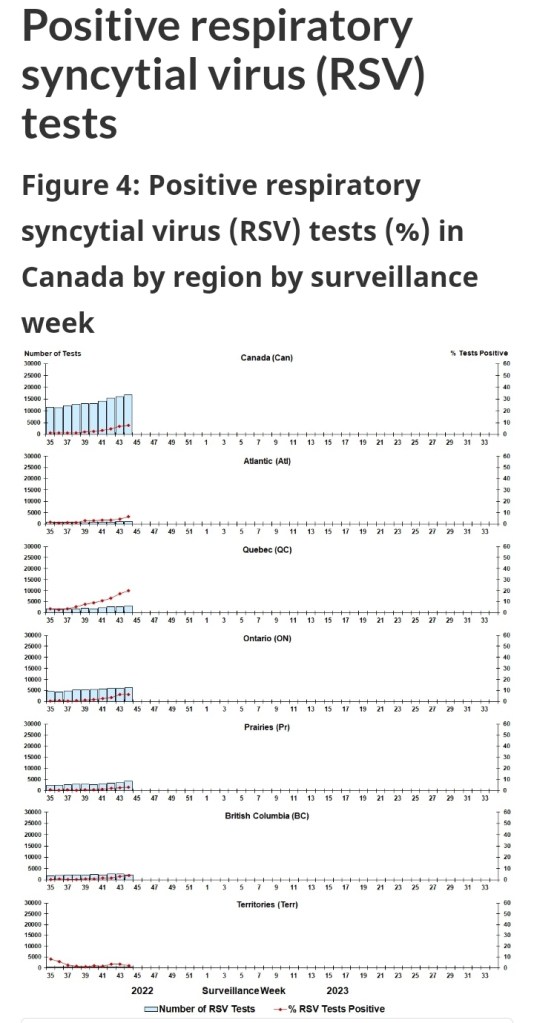
Public Health Canada’s Respiratory Virus Report first noted an unseasonable rise in RSV in the week ending 8 October 2022. The situation grew out of control within 4 weeks, with RSV test positivity rising to 20.1% in Quebec.
How did the Health Minister respond to doctors urging an RSV mask mandate? “Mask wearing is a personal choice in Ontario.”
Health Minister Jones made the Government’s plans very clear when she said that their goal was to have the healthcare system at “full capacity.” This means no reserve labour or resources, no flexibility or surge capacity for any outbreaks, no rest for doctors or nurses, no relief for anyone in the system. The explicit goal of the Ford government is to push the healthcare system to its absolute limit when there are still more waves of contagion about to crash into it.
What is Premier Ford’s solution to the problem of public healthcare? To cut even deeper and bleed it dry:
According to the Business Plan for Ontario Health, the “super-agency” created by Doug Ford in 2019 to find “efficiencies” in the health system, the system is actually spending too much.
From PressProgress.
Thousands of preventable infections and hospitalizations are the direct result of government policy. Children and adults are dying of illnesses and injuries which could have been treated at adequately staffed hospitals. The Ford Government deliberately aggravates the public health crisis and obstructs any remedy; they are responsible for the suffering and deaths caused by these epidemics.
[ Featured image from CBC, “Doug Ford swallowed a bee while talking about the possibility of privatizing health care.” 12 August 2022. ]
